

#ACA 2.0's sausage-making continues...will Medicare gain dental, vision, hearing & MOOP??
Tue, 04/06/2021 - 6:31pm
This is mostly an updated version of a post from last week, but there's some important new (potential) developments. Via Amy Lotven of Inside Health Policy:
The White House is expected to roll out the health care priorities for its two-part infrastructure package sometime this Spring, and the health piece potentially could move separately now that the Senate parliamentarian has agreed Democrats have another shot passing their priorities through a simple majority. While there appears to be consensus that the bill will expand, or make permanent, the Affordable Care Act tax credits from the American Rescue Plan, other policies are less clear and will likely depend on the amount of offsets lawmakers can glean from drug-pricing measures.
EXCELLENT! This doesn't specify whether it would be the dramatic expansion of APTC subsidies only (which would already be a huge upgrade), or whether it would also include the other ACA subsidy provisions included in Sen. Shaheen's S.499 (*see below), but it's still heartening to hear that the permanent APTC expansion, at least, appears to be baked in.
Some Democrats have talked of lowering the Medicare age to 60 or younger and adding vision, dental and hearing benefits, which would carry a hefty price-tag, while others say Congress should focus on finding a way to cover the millions of Americans with no insurance due to their states’ refusal to expand Medicaid.
In fact, some sources watching the discussions say the highest priority should be addressing the gap that keeps some of the most vulnerable Americans who make less than the poverty level from coverage since they’re neither eligible for Medicaid nor ACA subsidies.
All of these are important and any of them would be welcome improvements, but the Medicaid Gap is probably the most vexing because there's absolutely nor sane reason for it to still exist at this point. The ARP already offers a $16 billion flat-out BRIBE to the remaining non-expansion states into doing what they should've done seven years ago and most of them are still likely to blow it off, as Missouri and Wyoming have already proven.
...In 2019, House Democrats passed a bill (H.R. 3) that would let Medicare negotiate certain drugs, limit Part D and Part B price increases to inflation, require transparency and more. According to the Congressional Budget Office (CBO), the drug negotiations would save $456 billion over 10 years while capping prices at inflation would save about $36 billion.
House Democrats that year used the savings to pay for legislation adding dental, vision and hearing benefits to Medicare, at a total cost of $358 billion. That bill also redesigned the Part D program and capped out-of-pocket spending, at a cost of $9 billion over 10 years, and expanded Medicare’s program for low-income beneficiaries, which cost $105 billion. But the bill went nowhere in the then GOP-controlled Senate.
Assuming those numbers are still valid two years later, that'd be $472 billion in extra spending minus $492 billion in savings, for a net savings of $20 billion.
...In June 2020, House leadership again turned to H.R. 3. But this time they used the savings to offset their massive ACA improvement bill (H.R. 1425), which, among dozens of other policies, increased and expanded the ACA tax credits in the same way as the temporary measures in the newly enacted American Rescue Plan. But the 2020 bill also stalled in the Senate. CBO estimated at the time the enhanced tax credits would cost about $212 billion over 10 years.
That's the first time I've seen a mention of the CBO score for HR 1425. This score also projected that fixing the ACA's Family Glitch via legislation would tack on around $45 billion of federal spending. As Lotven noted yesterday, if the Biden Administration is able to do this via IRS regulatory changes, it wouldn't be counted at all as part of a formal CBO score.
Sources say congressional Democrats now also plan to glean offsets by repealing the Trump administration’s Medicare Part D rebate ban rule, which CMS’ actuary has said would cost about $196 billion if implemented.
Pelosi said recently that lowering the Medicare age and a public option are on the table for the next bill. But whether either could pass is a far different story.
I've already stated before that while Biden campaigned on both a Public Option and lowering the Medicare age to 60, each of them would face a steep uphill challenge...and unless the PO included strict, robust rate setting provisions, it's uncertain how much good it would actually do. Honestly, the biggest argument in favor of the PO at the moment is that it would resolve the Medicaid Gap...but so would eliminating the ACA's lower-bound 100% FPL subsidy cliff, really. Of course that would also create some other problems.
...The source has heard the legislation will definitely expand the enhanced ACA tax credits and pay for doing so by repealing the Part D rebate ban rule.
...One source says if there is not enough funding for the Medicare expansions and the ACA tax credit increases, lawmakers could craft a third solution that Biden also supports: capping out-of-pocket spending in Part D and expanding help for low-income beneficiaries.
Based on previous CBO scores, such a package would cost about $336 billion.
As you can see, there's a lot of moving parts at play here. The possible healthcare system improvements discussed in the article include (but are not limited to):
- Permanently kill the ACA premium subsidy cliff
- Permanently enhance ACA premium subsidies
- Add dental, vision & hearing care to Medicare
- "Do something" to close the Medicaid Gap
- Lower Medicare buy-in age from 65 to 60
- Let Medicare negotiate drug prices
- Cap Medicare price increases at inflation rates
- Cap Out of Pocket drug spending for Medicare
- Adding a Public Option of some sort
- Expanding Medicare coverage for low-income beneficiaries
It sounds like the first two items are basically a lock, along with at least 3-4 of the other 8 bullets above...the question is which of them make the final cut.
*I know I keep reposting this, but I'm really hoping all of Sen. Jeanne Shaheen's S.499 is included:
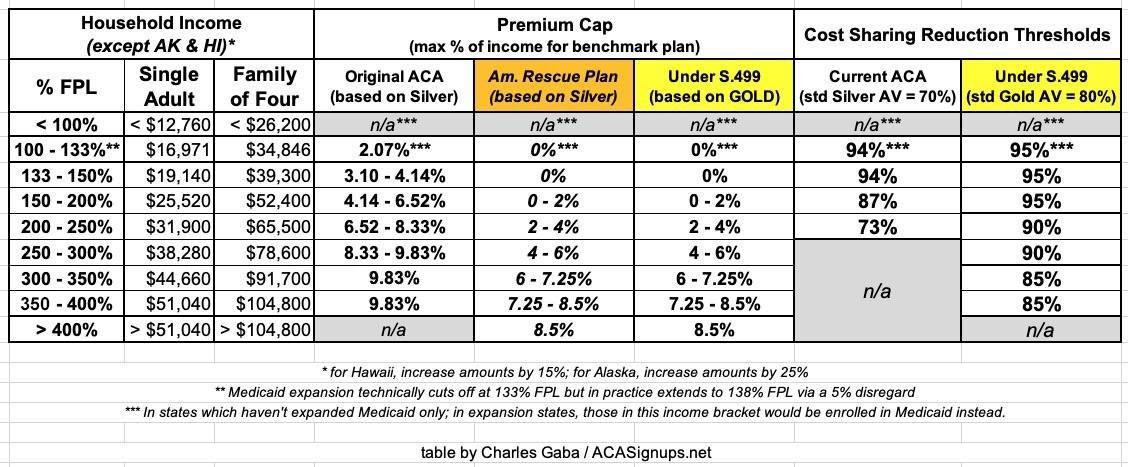
Senate Democrats led by New Hampshire Sen. Jeanne Shaheen are pushing legislation that would enhance the value of and eligibly for the Affordable Care Act’s cost-sharing reductions (CSRs) and permanently fund the program, thus eliminating the need for the “silver-loading” workaround that insurers crafted after the Trump administration ended direct payments to reimburse their costs for the subsidies in 2017.
...And the Senate Democrats’ bill would lift the actuarial value of the ACA subsides from 70% to 80% by linking the premium tax credits to the gold-level instead of silver-level plans.
...It also would expand CSRs to everyone earning up to 400% of poverty. For enrollees earning up to 200% FPL, the CSRs would hike the actuarial value of their plan from 87% up to 95%. Enrollees earning 200%-300% of FPL would have plans with a 90% AV and those earning from 300%-400% of FPL would get their plan value boosted to 85% AV.
Here, again, is a table summarizing how the current ACA subsidy structure works for both premiums and cost sharing (deductibles, co-pays & coinsurance); how the American Rescue Plan has temporarily beefed up the premium subsidies; and how both would look under S.499's permanently expanded subsidy structure for both premiums & cost sharing reductions:
Advertisement
