Many of the findings were things which I had been either predicting or documenting all year:
Enrollment through Healthcare.gov Was 5 Percent Lower in 2018 than 2017
Stakeholders Reported That Plan Affordability Likely Played a Major Role in Enrollment
HHS Reduced Consumer Outreach for 2018 and Used Problematic Data to Allocate Navigator Funding
HHS Did Not Set Numeric Enrollment Targets for 2018, and Instead Focused on Enhancing Certain Aspects of Consumers’ Experiences
We identified a list of factors that may have affected 2018 healthcare.gov enrollment based on a review of Department of Health and Human Services information, interviews with health policy experts, and review of recent publications by these experts related to 2018 exchange enrollment.
Azar Says He Is Not Aware Of Discussions On Blocking ‘Silver-Loading’ in 2019
HHS Secretary Alex Azar said that he has not been involved in discussions about blocking ‘silver-loading’ plans in 2019 and is not aware of any agency discussions about ending the practice at the moment.
...In recent weeks, some stakeholders have speculated that the Trump administration could block silver-loading in 2019. Several pro-ACA experts say that even though the administration may have authority to stop silver-loading, it would be a self-destructive move, especially leading up to the November midterm elections.
CMS Administrator Seema Verma told reporters on Thursday (March 22) that she was “very concerned” about certain aspects of ‘silver loading’ plans, namely that it raises costs for unsubsidized consumers and the federal government. Verma did not commit to allowing or blocking the process for the 2019 plan year.
This year, thanks to their reinsurance program, ACA individual market premiums dropped by around 23.6% on average, from a whopping $1,040/month to "only" $795/month per enrollee.
No Load: They could gamble that the CSR problem would be resolved and the payments would be made after all (i.e., they would price normally).
Broad Load: They could spread the CSR cost out evenly across all of their 2018 ACA policies, on exchange & off.
Silver Load: They could load the CSR costs onto all Silver plans only (both on & off exchange).
Silver Switcharoo: They could load CSR costs onto all on-exchange Silver plans only, while also creating "mirror" Silver plans off-exchange without any CSR load.
Mixed Load: Each insurance carrier could choose whichever of the other 4 strategies they wanted to and let the chips fall where they may. Not sure if this really counts as a "strategy", since it's more or less "all of the above".
For nearly a year, healthcare wonks like myself, David Anderson, Andrew Sprung and Louise Norris have been heavily getting the word out to promote not just the "Silver Loading" CSR-load workaround, but an even more clever variant which I've coined "the Silver Switcharoo" which takes the concept of Silver Loading and goes one step further.
20 states went the full #SilverSwitcharoo route (the best option, since it maximizes tax credits for those eligible for them while minimizing the number of unsubsidized enrollees who get hit with the extra CSR load);
16 states went with partial #SilverLoading (the second best option: Subsidized enrollees get bonus assistance, though not as much as in Switch states; more unsubsidized enrollees take the hit, but they aren't hit quite as hard);
6 states went with "Broad Loading", the worst option because everyone gets hit with at least part of the CSR load except for subsidized Silver enrollees;
6 states took a "Mixed" strategy...which is to say, no particular strategy whatsover. The state insurance dept. left it up to each carrier to decide how to handle the CSR issue, and ended up with a hodge podge of the other three
3 states (well, 2 states + DC, anyway) didn't allow CSR costs to be loaded at all. Their carriers have to eat the loss, which makes little sense, but what're ya gonna do?
Implications Of CMS Mandating A Broad Load Of CSR Costs
In October 2017, the Trump administration eliminated federal funding to reimburse insurers for cost-sharing reduction (CSR) subsidies, which they are obligated to provide to qualifying enrollees in the Affordable Care Act (ACA) Marketplace. President Donald Trump had threatened to eliminate CSR funding throughout 2017, so insurers and insurance regulators in many states had anticipated the move by adding the cost of CSRs to premiums for 2018.
Louise Norris is an awesome source for all sorts of healthcare policy/insurance data, but she's especially on top of developments in her home state of Colorado, where she and her husband Jay run a small brokerage outlet.
Today Jay and Louise have a couple of interesting tidbits out of The Centennial State (yeah, I had to look up their nickname myself).
That's (sort of) an 88% retention rate through early May. I say "sort of" because this presumably includes some amount of churn (if 100 people drop coverage and 100 off-season enrollees sign up, that'd be a net change of zero). Even so, it's actually slightly better compared to prior years, when the national effectuation number had usually dropped to around 87% by the end of March.
The Affordable Care Act (ACA), in section 1402, requires insurers who participate in the marketplaces established under that act to offer CSRs to eligible people who purchase silver plans through the marketplaces. CBO views that requirement as establishing an entitlement for thoseeligible.
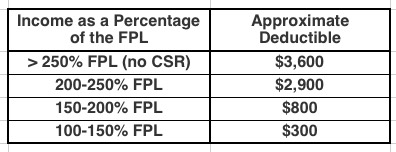
To qualify for CSRs, people must purchase a plan through a marketplace and generally have income between 100 percent and 250 percent of the federal poverty guidelines (also known as the federal poverty level, or FPL). The size of the subsidy varies with income.
CSRs reduce deductibles and other out-of-pocket expenses like copayments. For example, in 2017, by CBOs estimates, the average deductible for a single policyholder (for medical and drug expenses combined) with a silver plan varied according to income in the followingway: