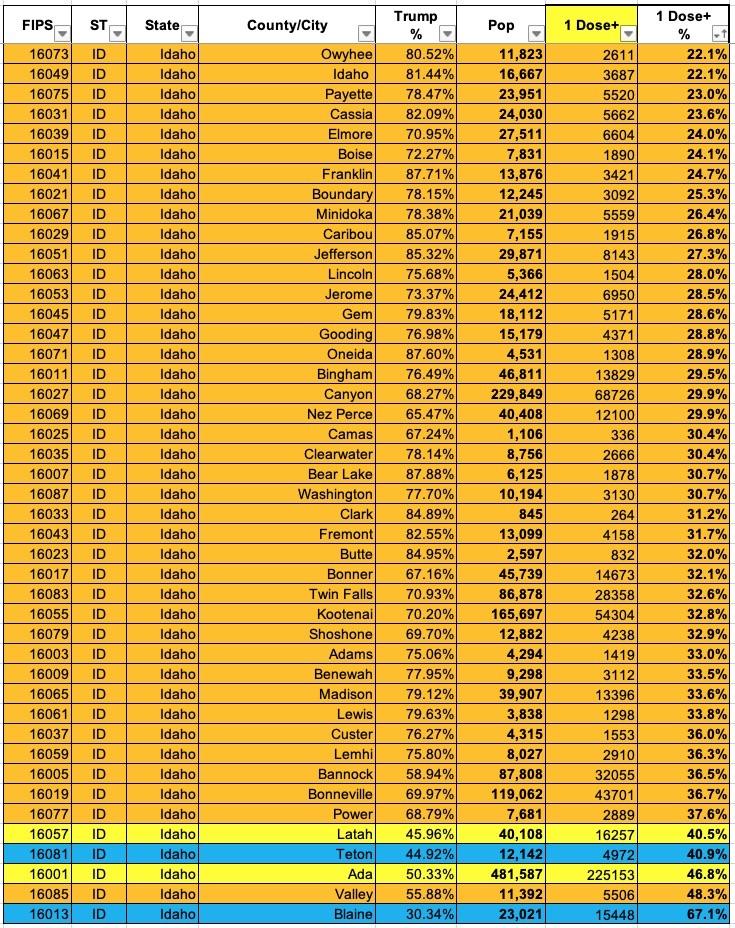
Now that I've developed a standardized format/layout & methodology for tracking both state- and county-level COVID vaccination levels by partisan lean (which can also be easily applied to other variables like education level, median income, population density, ethnicity, etc), I've started moving beyond my home state of Michigan.
The ACA was originally designed with the intention that all documented Americans living in all 50 states (+DC) earning up to at least 138% of the Federal Poverty Level (FPL) would be eligible for Medicaid. Unfortunately, the 2012 NFIB v. Sebelius ruling by the U.S. Supreme Court stated that Medicaid expansion under the ACA had to be left up to each individual state.
This meant that each state had to decide, whether by legislation, executive order (depending on the state) or ballot initiative, whether or not to expand the low-income public health program or not. Under the ACA, any state which does so will have 90% of the cost paid for by the federal government, while the state has to pony up the other 10% of the cost.
Mississippi once again has two carriers offering ACA-compliant individual market coverage in 2021 and six on the small group market. Unfortunately, few filing forms don't seem to be available and the ones which are are redacted, so I can't run weighted averages for either.
The unweighted average rate increases are 2.7% on the individual market and basically flat for small group plans.
For the past two weeks, along with other noteworthy Open Enrollment data numbers, I've been scratching my head over what the deal is in Mississippi:
Once again, Maine remains the worst-performer year over year, mostly due to their expansion of Medicaid. Idaho isn't listed because they're a state-based exchange and haven't reported any data yet. Mississippi, on the other hand, continues to be the top out-performer vs. last year, which is interesting because there doesn't seem to be any particular reason for it.
Unlike some states, Mississippi hasn't implemented any additional subsidies, a mandate penalty or a reinsurance program of any sort. They haven't had any new carriers join the ACA market, nor have any of them left. I don't think either of the carriers on the exchange have significantly expanded their territory or changed their offerings that much either...in fact, average premiums are essentially flat year over year.
In other words, by all rights, Mississippi should be performing almost exactly as they did last year...but enrollments are up 15.5% to date. Huh.
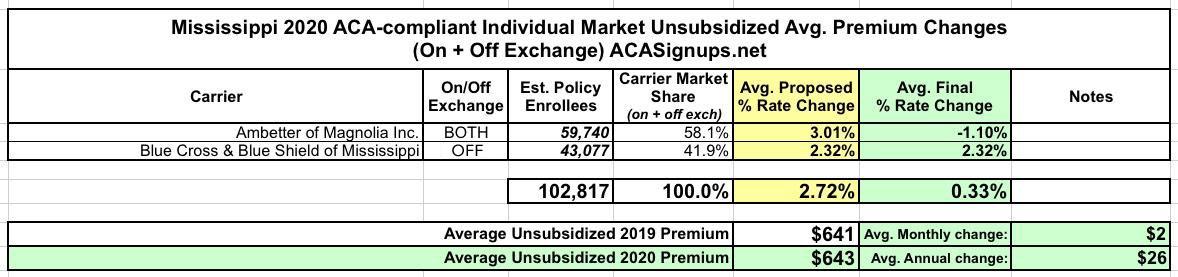
Mississippi once again has two carriers offering ACA-compliant individual market coverage in 2020: Ambetter of Magnolia, which holds 58% of the market, and Blue Cross Blue Shield with the other 42%. Earlier this year they were asking for average rate hikes of 3.0% and 2.3% respectively, but Ambetter's final/approved rates are coming in at a 1.1% reduction, bringing the overall average down to a mere 0.3% rate hike.
OK, my math here is gonna be a bit sloppy, but I'm just trying to illustrate a larger point about how splitting risk pools is, generally speaking, a Bad Thing.
Under the Affordable Care Act, non-ACA compliant healthcare policies were given until December 31st, 2013 to become fully ACA-compliant, including the new regulations mandating guaranteed issue, community rating, essential health benefits, no more annual or lifetime limits on coverage and so forth. All major medical policies offered from that day forward had to be fully ACA compliant (although there were some exceptions for short-term plans and so forth).
However, there was an exception made: Any existing policy which someone had been continuously enrolled in since before the ACA was signed into law by President Obama in March 2010 was considered to be "grandfathered" in. As long as the insurance carrier chose to keep offering those non-compliant policies, existing enrollees could remain enrolled, although premiums would of course increase from time to time. The "locked in" pool of enrollees would gradually dwindle as enrollees died, aged onto Medicare, got jobs with employer coverage and so on.
But that's not all! In addition to the actual 2018 MLR rebates, I've gone one step further and have taken an early crack at trying to figure out what 2019 MLR rebates might end up looking like next year (for the Individual Market only). In order to do this, I had to make several very large assumptions:
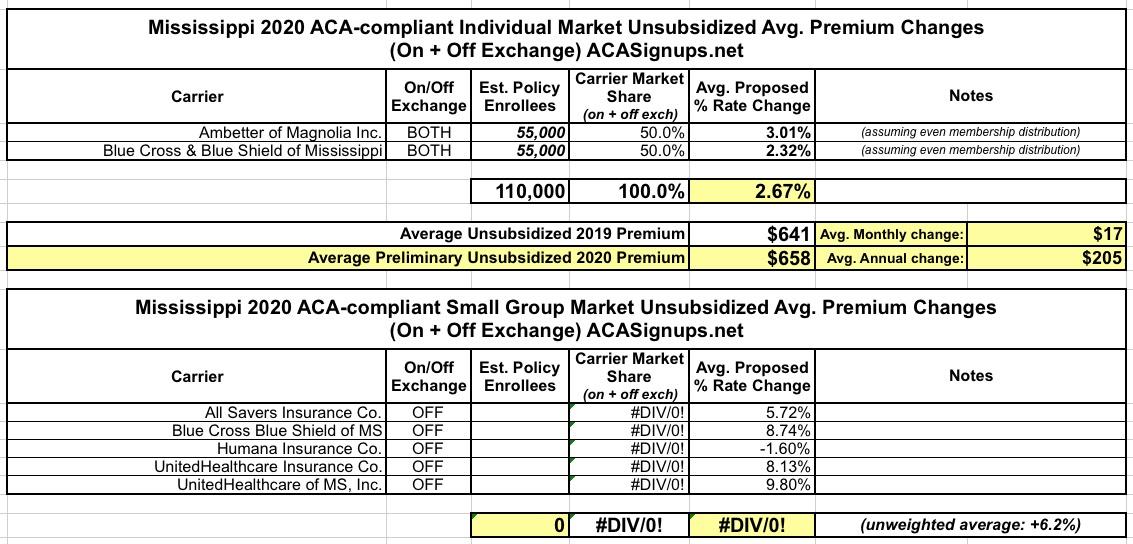
As a result, I have no idea what the relative market share is between the two and am assuming they're roughly even. Even if they aren't, the requested rate changes are so close it doesn't make much difference anyway (2.3% and 3.0%). If approved as is, unsubsidized Mississippians can expect to pay about $200 more total next year.
On the small group market, there's five carriers; again, I don't know the market share of any of them, so the unweighted average increase is 6.2% statewide.
I realize this may seem a bit late in the game seeing how the 2019 ACA Open Enrollment Period has already started, but I do like to be as complete and thorough as possible, and there were still 9 states missing final/approved premium rate change analyses as of yesterday which I wanted to check off my 2019 Rate Hike Project list.
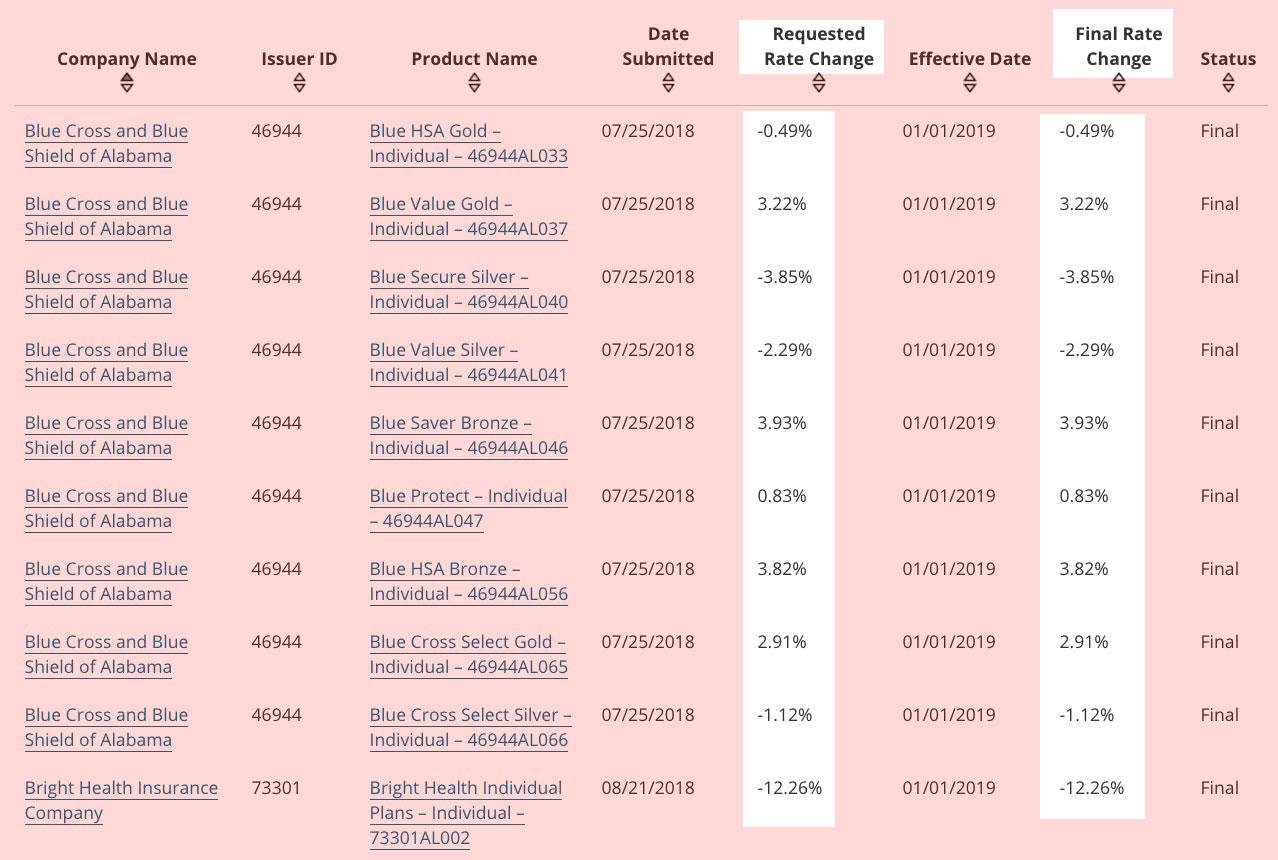
Fortunately, RateReview.HealthCare.Gov has finally updated their database to include the approved rate changes for every state, which made it easy to take care of most of these. Making things even easier (although not necessarily better from an enrollee perspective), in three states the approved rates are exactly what the requested rates were for every carrier: Alabama, Mississippi and Utah:
Mississippi is pretty easy: Only two carriers. I have no idea what their relative market share is (the enrollment data along with a lot of other stuff is redacted in their filings), but in this case it really doesn't matter because both of the carriers are requesting nearly identical rate changes anyway...which is to say, just about no change whatsoever.
The Urban Institute projected that #MandateRepeal and #ShortAssPlans would add a 17.2 percentage point rate hike factor in Mississippi. I generally knock 1/3 off of their estimates to err on the side of caution (11.4%), but given Ambetter specifically stating that they didn't add any increase to account for #ShortAssPlans (why?? interesting!), I'm shaving off a bit more and assuming a flat 10% impact.
This means that unsubsidized Mississippi enrollees would likely have saved a good $800 apiece next year without Trump/GOP efforts to undermine the ACA this year.




{kind=link}