

Whether "Medicare for All" or "Medicare for More", there's another big nut which would have to be cracked.
Wed, 02/06/2019 - 7:08pm
In U.S. politics, the Hyde Amendment is a legislative provision barring the use of federal funds to pay for abortion except to save the life of the woman, or if the pregnancy arises from incest or rape. Legislation, including the Hyde Amendment, generally restricts the use of funds allocated for the Department of Health and Human Services and consequently has significant effects involving Medicaid recipients. Medicaid currently serves approximately 6.5 million women in the United States, including 1 in 5 women of reproductive age (women aged 15–44).
Federal dollars can't be used to pay for abortion outside of the above restrictions, but Medicaid is funded via hybrid federal/state funding, so there are 15 states where Medicaid does pay for abortion using the state's portion of the funding.
The Hyde Amendment has popped up as an issue many times, and I've written about it more than a few times even in cases where I didn't mention it directly, such as this post regarding Planned Parenthood funding, but I've obviously mainly focused on writing about Hyde as it relates to the Affordable Care Act.
When attempting to get the ACA passed back in 2010, Congressional Democrats ran into a problem with anti-choice Democrats (as well as Republicans, of course, not that any of them voted for it anyway) when it came to the two types of federal financial assistance provided to ACA exhange enrollees: Advanced Premium Tax Credits (APTC) and Cost Sharing Reductions (CSR).
The problem is that unlike Medicaid, APTC and CSR both use 100% federal dollars, and under Hyde can't be used to pay for abortions. Since some ACA exchange policies include abortion coverage, anti-choice forces claimed that some of the subsidy funding would be used to pay for them, running afoul of Hyde. And so, an absurdly complicated workaround was developed and grudgingly agreed to:
The ACA allows the coverage of abortion services through the marketplaces but includes a number of restrictions and requirements that insurers must follow before covering non-Hyde abortions. Many, though not all, of these restrictions are outlined in Section 1303 of the ACA, which includes specific rules related to the coverage of abortion services by QHPs and has been the subject of previous litigation. In particular, Section 1303:
- Prohibits insurers from using any portion of premium tax credits or cost-sharing reduction payments to pay for non-Hyde abortion services;
- Requires insurers to inform consumers in their summary of benefits and coverage that the QHP they are considering includes coverage of non-Hyde abortion services; and
- Requires insurers that cover non-Hyde abortions to determine the cost of and then separately collect and segregate funds for non-Hyde abortion services.
Section 1303 further specifies that individuals who purchase insurance that covers abortions must pay at least one dollar into a separate account specifically designated for abortion. These segregated accounts are designed to help ensure that the accounts are 1) funded solely by the enrollee’s premium (rather than by the premium tax credit) and 2) used exclusively to fund non-Hyde abortion services. Section 1303 also allows states to ban the coverage of abortions by QHPs sold through the marketplaces: to date, twenty-six states have done so. In an additional six states, no marketplace plans offered coverage for abortion during the 2016 plan year. Two states—California and New York—require health plans to cover abortions, subject to an exception for multistate plans, at least one of which in each state must offer insurance without abortion coverage.
As I noted over a year ago, this has led to an incredibly convoluted situation:
To further address these concerns, CCIIO’s bulletin reminds QHP issuers of their ongoing obligations under Section 1303 to 1) not seek premium tax credit payments or cost-sharing reduction reimbursement for coverage of non-Hyde abortion services; 2) provide an annual notice in the summary of benefits and coverage that describes whether non-Hyde abortion services are covered by the QHP; and 3) charge and collect no less than $1 per enrollee per month for coverage of non-Hyde abortion services and deposit such amounts collected into a separate allocation account that is used exclusively to cover non-Hyde abortions.
That's right: All ACA exchange enrollees in policies which cover abortion have $12 per year of their premiums separated out by the insurance carrier and deposited into a separate bank account, where the money just sits there to only be used for any abortion claims which might come up.
At the time, I did a little back-of-the-envelope math and realized that only around 13% of that money is likely ever actually used to pay for an abortion each year, which means that there's probably well over $100 million just sitting gathering dust (and interest) in various "Abortion Funds" throughout the country, legally prohibited from ever being used for anything other than abortions until the end of time (or the end of the ACA, anyway).
Then, last November, things got even more surreal on the Hyde/ACA front:
Trump administration proposes new rule requiring separate premium bills for abortion coverage
The Trump administration wants insurers that offer plans through Access Health CT, Connecticut’s Affordable Care Act exchange, and other exchanges nationwide, to send people separate monthly bills for the cost of their abortion coverage — in addition to the bill they get for their regular premium costs.
This means people would receive two separate bills in the mail or electronically — one to cover the premium costs for services such as primary care, mental health, maternity, etc. — and another one solely for the cost of their abortion coverage premium.
People on the exchange would also have to make two separate payments for these bills, according to a proposed rule recently released by the Centers for Medicare and Medicaid Services (CMS).
Yes, that's right: The Trump Administration is now insisting that insurance carriers send out separate bills for $1.00 per month per enrollee, specifically for "Abortion Services" or whatever the euphemistic language they decide to go with is. Between printing, postage, processing and so forth, there's a good chance it will cost the carriers more than $1.00 per enrollee anyway, which will lead some of them to drop abortion coverage from their policies altogether, which is of course the entire point.
In addition, this will humiliate and embarrass many women enrolled in the policies as they're further degraded by having an extremely personal and sensitive medical issue specifically called out. And of course I'm pretty sure thousands of people will end up receiving late payment notices (potentially even losing their coverage eventually) even when they pay their premiums regularly because they didn't notice the second invoice for a mere $1.00 that shows up each and every month.
This policy was supposed to go into effect on January 1st, 2019. I'm looking into whether or not this has actually been implemented yet and will update once I find out.
HOWEVER...none of the above is the actual point of this entry. Everything I've written until now is just to drive home how insanely controversial and difficult it is to craft and implement federal healthcare policy around abortion as long as the Hyde Amendment is part of the equation.
Well, it's about to get a whole lot worse.
In 2016, the Hyde Amendment played a major role in the downfall of a state-based Single Payer ballot proposal. The state of Colorado voted on a partial SP bill called ColoradoCare, which (if it had become law) would have been funded partly by repurposing federal funds for Medicare, Medicaid and the ACA and partly using state funding. Here's what happened:
Last November the residents of Colorado had the opportunity to pass a Single Payer healthcare bill at the state level. If it had passed, about a quarter of the population would've stayed put, but everyone else would've been covered with a new Single Payer system, paid for partly with Obamacare funding and partly by adding new payroll and income taxes. Remember, these taxes would be replacing just about all of the payments that Colorado residents are currently paying for their health insurance.
Bernie Sanders campaigned for the Colorado plan. So did Michael Moore, Noam Chomsky, and other progressive big shots. Colorado is a purple-to-blueish state. You would think that it would've either passed or, at worst, come kinda close. Instead, the proposal was spin-kicked right in the suckhole.
Now, you can argue that opposition from a couple of Colorado's highest profile Democratic officials didn't help matters ... but it still lost 80 to 20 in a state where Hillary Clinton won by five points. On paper, it should've gotten a hell of a lot more than 20 percent of the vote ... but in practice, it was simply too big a shock to the system all at once for people to swallow, even if the numbers added up.
There were a lot of reasons why ColoradoCare was crushed, but one of them was this:
The ballot campaign to create universal health care in Colorado drew an unlikely and prominent opponent this week: NARAL ProChoice Colorado, one of the state’s leading abortion rights groups.
The organization — more accustomed to fighting to expand health care services — is opposing Amendment 69 because it worries that the measure could limit access to abortion care.
Under NARAL’s legal interpretation, a constitutional ban on using “public funds” for abortion approved by voters in 1984 would prohibit Colorado Care from covering the procedure because it would be a political subdivision of the state.
The Vote Yes group contested that interpretation, but it didn't matter; NARAL said no dice, since if they were correct there would be no funding for abortions from either the feds or the state, leaving 3/4 of the women of Colorado left to fend for themselves.
You can see where I'm going with this now, I'm sure.
Both the "Medicare for All" Senate Bill 1804 sponsored by Sen. Bernie Sanders and co-sponsored by more than a dozen Democratic Senators and the "Medicare for America" bill co-sponsored by Rep. Rosa DeLauro and Rep. Jan Schakowsky would explicitly cover full reproductive and maternity services.
Here's the wording in S.1804 (Medicare for All) for how it would deal with Hyde:
(3) RESTRICTIONS SHALL NOT APPLY.—Any other provision of law in effect on the date of enactment of this Act restricting the use of Federal funds for any reproductive health service shall not apply to monies in the Trust Fund.
Medicare for America uses the same wording but adds another entry to underscore the point:
‘(c) RESTRICTIONS SHALL NOT APPLY.—Any other provision of law in effect on the date of enactment of this title restricting the use of Federal funds for any reproductive health service, including abortion, shall not apply to monies in the Trust Fund.
...SEC. 127. ABORTION COVERAGE. Notwithstanding any other provision of law, Federal funds may be used to provide for abortion services under any health program under any of the following: (1) Indian Health Service. (2) Benefits provided to women veterans. (3) Benefits provided through the United States Immigration and Customs Enforcement to women in detention centers under the jurisdiction of such agency.
So...OK. They've crossed their T's and dotted their I's legislatively. Neither bill technically repeals Hyde, they just say that it "shall not apply" to the funding of MFA/Med4America, which I assume is Constitutionally valid. This would effectively leave Hyde technically still in place but functionally toothless, in much the same way that the ACA's individual mandate penalty is still technically on the books but set to $0.
This is incredibly important, of course, because assuming either one of these ever actually becomes the law of the land, they would be the only game in town for abortion coverage for anyone enrolled in the program. This is a bigger deal for S.1804, of course, since it would theoretically cover everyone in the country, but it'd still apply to a good 50% or more of the population under Medicare for America (the other half of the population would still be covered under private employer-based policies).
Politically, however, there will be a major firestorm over Hyde regardless of which universal coverage bill ends up going forward. The Democratic Party (especially the women within it) seem ready to take on that fight...but it's gonna be ugly as hell even apart from the battle over the rest of the healthcare bill.
How is abortion (not including cases of rape, incest or life of the mother) handled by Medicare today?
Well, to know that, it's first helpful to know how many women covered by Medicare have abortions...and the answer isn't likely to be a lot. 84% of Medicare enrollees are over 65 to begin with (and therefore unlikely to become pregnant), which leaves around 9.1 million under 65, of which 47% are women, or around 4.3 million women with disabilities of child-bearing age.
The national abortion rate as of 2014 in the U.S. was 14.6 per 1,000 women of child-bearing age across the total population. That would translate into a maximum of 63,000 abortions per year among Medicare enrollees if extrapolated directly, although the rate is likely considerably lower among those with long-term SSDI, ALS or ESRD. Let's call that a high water mark.
I assumed that there was no way that Medicare would possibly pay for abortions except, again, in cases of rape, incest or the life of the mother...
...until last night, when my friend and colleague Joshua Schultz forwarded me one hell of an eyebrow-raising document that he stumbled across awhile back.
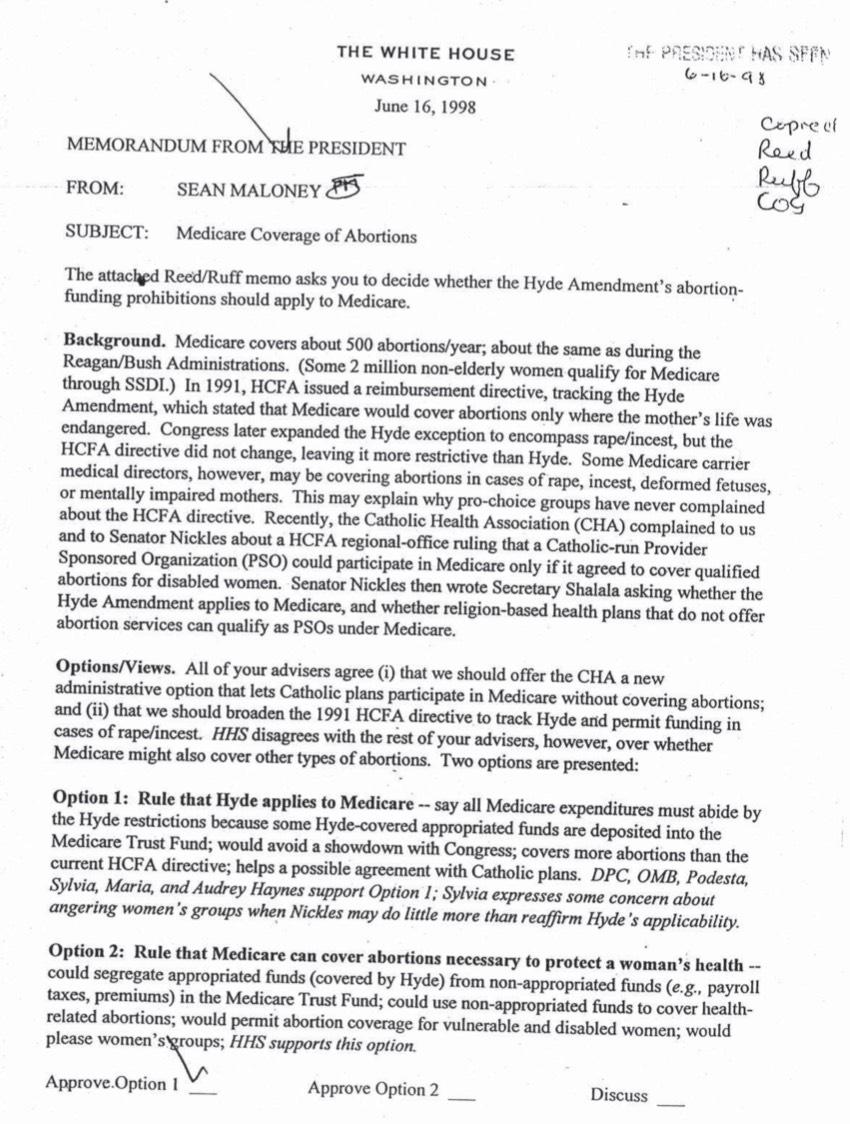
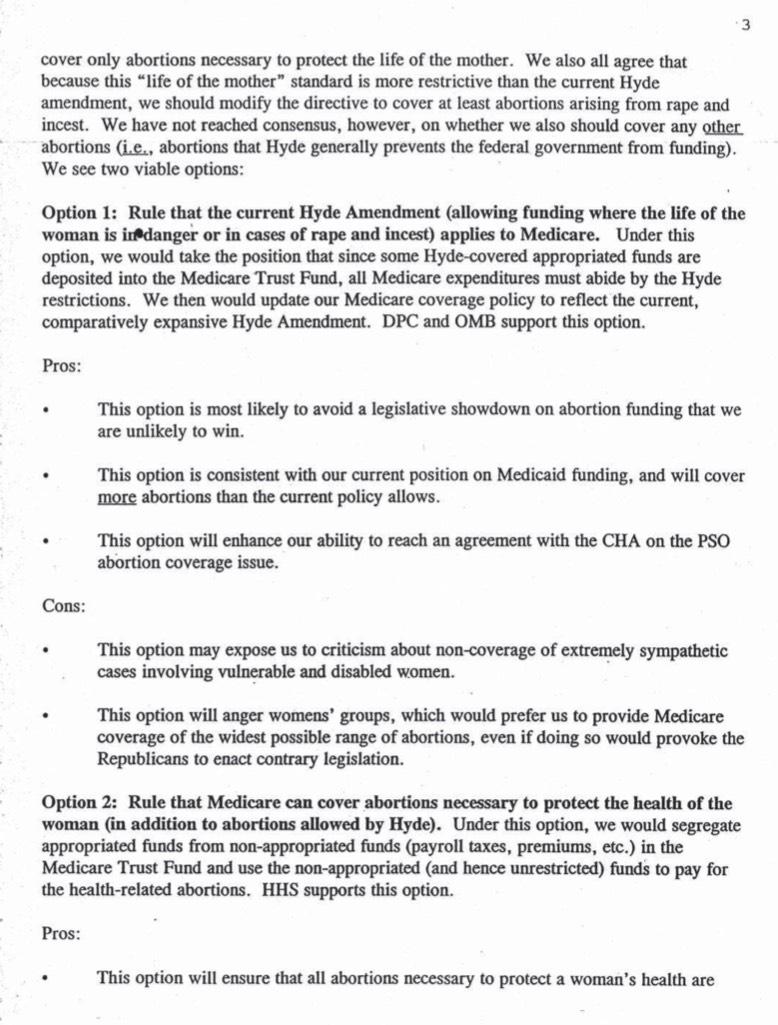
Aside from anything else, this at least answers my original question: Around 500 abortions per year were covereed under the Reagan, Bush and Clinton administrations out of roughly 2 million women under 65 enrolled in Medicare. That presumably translates into around 1,100 per year today.
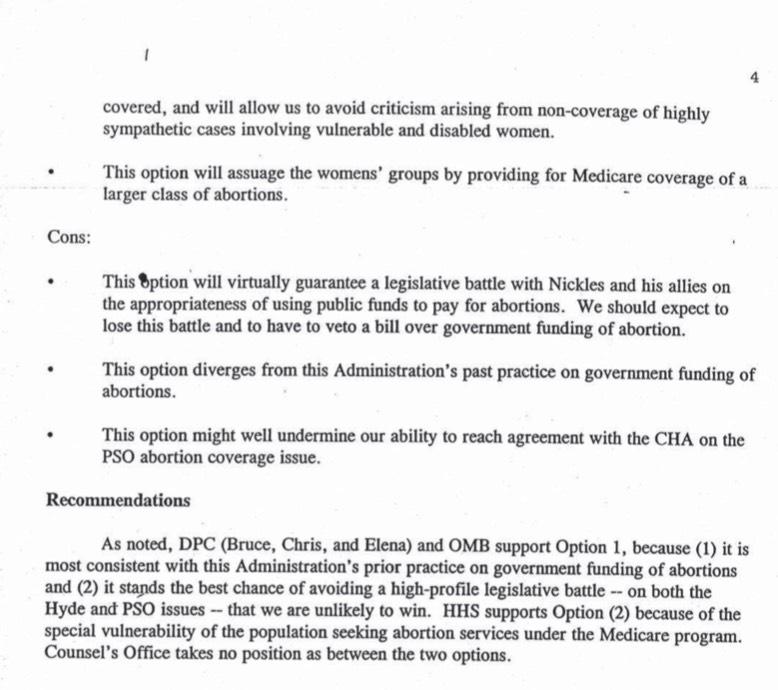
President Clinton ultimately approved "Option 1", which used a strict interpretation of Hyde for Medicare enrollees. As noted in the memo, this was less restrictive than the prior directive (life of the mother only) but more restrictive than how it had apparently been handled up until that point (life of the mother, health of the mother, rape, incest, deformed fetuses & mentally impaired mothers (the full memo clarifies that there were 700,000 seriously mentally impaired women of childbearing age on Medicare at the time...which means if they were pregnant, it would have to be due to their being raped).
The other thing which I find noteworthy is the description of "Option 2": "Secgregate appropriated funds from non-appropriated funds in the Medicare Trust Fund; could use non-appropriated funds to cover health-related abortions/etc". That sounds awfully famliar...in fact, that's exactly the workaround that the ACA came up with and utilizes today. For all I know this unused "Option 2" could even be where they got the idea in the first place.
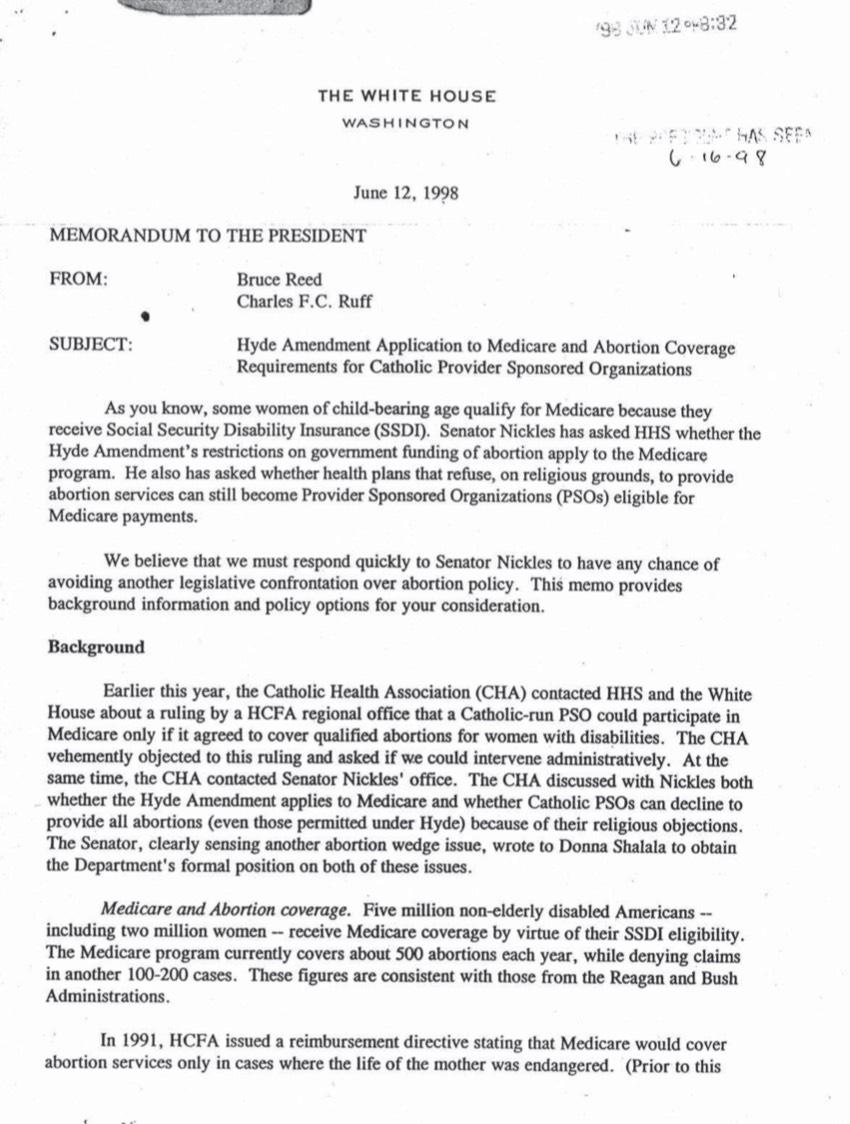
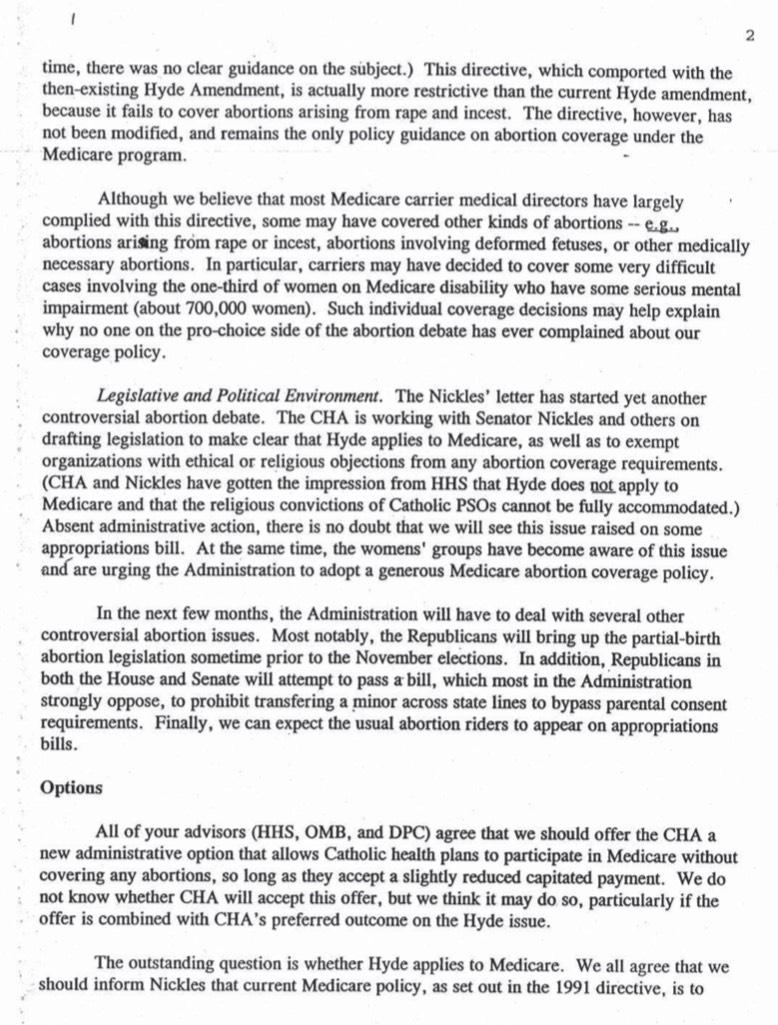
Here's the memo itself, which includes some additional noteworthy items. For the record, "Sen. Nickles" appears to be former Republican U.S. Senator Don Nickles of Oklahoma. Donna Schalala, of course, was Pres. Clinton's HHS Secretary at the time, but was also just elected a freshman member of Congress from Florida's 27th District, in a nice bit of coming full circle:
A shout-out to Rebecca Barson for filling in the mystery of the remaining name:
This memo made the rounds a few years ago because “Elena” mentioned on page 4 is Elena Kagan. Also of note is this new GAO report about how many state Medicaid programs aren’t meeting their obligations to cover Hyde-mandated abortions: https://t.co/sqwPvjnVbE
— Rebecca Barson (@rdbarson) February 9, 2019
Elana Kagan, of course, is now a sitting U.S. Supreme Court Justice.
Advertisement
